Which of the following control measures is MOST effective in preventing transmission of Legionella in healthcare water systems?
Flushing all faucets with hot water for 5 minutes daily.
Maintaining hot water storage temperatures above 140°F (60°C).
Installing carbon filters on all hospital water outlets.
Routine testing for Legionella in hospital water.
Maintaining hot water at 140°F (60°C) prevents Legionella growth and is the most effective control strategy.
Flushing water (A) alone is not sufficient.
Carbon filters (C) do not remove Legionella.
Routine testing (D) is not always necessary unless an outbreak occurs.
CBIC Infection Control References:
APIC Text, "Waterborne Pathogens and Infection Control," Chapter 9.
The MOST important characteristic to include when using a template for a comprehensive annual risk assessment is
system strategic goals and objectives.
cost savings attributed to the infection prevention and control program.
facility specific demographics end healthcare-associated Infection data
statewide communicable disease and healthcare-associated infection data
A comprehensive annual risk assessment should focus on facility-specific factors, including patient population, infection trends, and operational risks.
Why the Other Options Are Incorrect?
A. System strategic goals and objectives – While important, goals should align with facility-specific infection risks.
B. Cost savings attributed to infection control – Cost considerations are secondary to risk assessment.
D. Statewide communicable disease and HAI data – Broader epidemiological data is useful but should complement, not replace, facility-specific data.
CBIC Infection Control Reference
APIC emphasizes that facility-specific infection data is essential for an effective risk assessment.
What method of evaluation will BEST identify a staff member’s competency with reprocessing medical devices?
Verbalize the importance of reprocessing.
Demonstrate the appropriate sterilization procedure.
Describe the facility’s sterilization policies and procedures.
Obtain a score of 100% on a post-test following a reprocessing course.
The correct answer is B, "Demonstrate the appropriate sterilization procedure," as this method of evaluation will best identify a staff member’s competency with reprocessing medical devices. According to the Certification Board of Infection Control and Epidemiology (CBIC) guidelines, competency in reprocessing medical devices—such as cleaning, disinfection, and sterilization—requires not only theoretical knowledge but also the practical ability to perform the tasks correctly and safely. Demonstration allows the infection preventionist (IP) to directly observe the staff member’s hands-on skills, adherence to protocols (e.g., AAMI ST79), and ability to handle equipment, ensuring that the reprocessing process effectively prevents healthcare-associated infections (HAIs) (CBIC Practice Analysis, 2022, Domain IV: Education and Research, Competency 4.3 - Assess competence of healthcare personnel). This method provides tangible evidence of proficiency, as it tests the application of knowledge in a real or simulated setting, which is critical for ensuring patient safety.
Option A (verbalize the importance of reprocessing) assesses understanding and awareness, but it is a theoretical exercise that does not confirm the ability to perform the task, making it insufficient for evaluating competency. Option C (describe the facility’s sterilization policies and procedures) tests knowledge of guidelines, which is a component of competence but lacks the practical demonstration needed to verify skill execution. Option D (obtain a score of 100% on a post-test following a reprocessing course) measures theoretical knowledge and retention, but a perfect score does not guarantee practical ability, as it does not assess hands-on performance or problem-solving under real conditions.
The focus on demonstration aligns with CBIC’s emphasis on assessing competence through observable performance, ensuring that staff can reliably reprocess devices to maintain a sterile environment (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.3 - Ensure safe reprocessing of medical equipment). This method supports a comprehensive evaluation, aligning with best practices for training and competency assessment in healthcare settings.
References: CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.3 - Ensure safe reprocessing of medical equipment; Domain IV: Education and Research, Competency 4.3 - Assess competence of healthcare personnel. AAMI ST79:2017, Comprehensive guide to steam sterilization and sterility assurance in health care facilities.
Which performance improvement model should the infection preventionist use to aid in the evaluation of the infection control plan?
Six Sigma
Failure mode and effects analysis
Plan, Do, Study, Act
Root Cause Analysis
The Plan, Do, Study, Act (PDSA) model is a widely used performance improvement tool in infection prevention. It focuses on continuous quality improvement through planning, implementing, analyzing data, and making adjustments. This model aligns with infection control program evaluations and The Joint Commission’s infection prevention and control standards.
Why the Other Options Are Incorrect?
A. Six Sigma – A data-driven process improvement method but not as commonly used in infection control as PDSA.
B. Failure Mode and Effects Analysis (FMEA) – Used to identify risks before implementation, rather than ongoing evaluation.
D. Root Cause Analysis (RCA) – Used to analyze failures after they occur, rather than guiding continuous improvement.
CBIC Infection Control Reference
The PDSA cycle is a recognized model for evaluating and improving infection control plans.
In the current year, cases of tuberculosis (TB) among foreign-born persons accounted for the majority of new TB cases in the United States. The number of states with greater than 50% of cases among foreign-born persons increased from four cases ten years ago to 22 cases in the current year. This information can BEST be used to
heighten awareness among Emergency Department staff.
inform staff who are foreign-born.
educate patients and visitors.
review the TB exposure control plan.
1 and 2 only.
1 and 4 only.
2 and 3 only.
3 and 4 only.
The correct answer is B, "1 and 4 only," indicating that the information can best be used to heighten awareness among Emergency Department (ED) staff and review the TB exposure control plan. According to the Certification Board of Infection Control and Epidemiology (CBIC) guidelines, tuberculosis (TB) remains a significant public health concern, particularly with the increasing proportion of cases among foreign-born persons in the United States. The data showing a rise from four to 22 states with over 50% of TB cases among foreign-born individuals highlights an evolving epidemiological trend that warrants targeted infection prevention strategies (CBIC Practice Analysis, 2022, Domain II: Surveillance and Epidemiologic Investigation, Competency 2.1 - Conduct surveillance for healthcare-associated infections and epidemiologically significant organisms).
Heightening awareness among ED staff (option 1) is critical because the ED is often the first point of contact for patients with undiagnosed or active TB, especially those from high-prevalence regions. Increased awareness can improve early identification, isolation, and reporting of potential cases. Reviewing the TB exposure control plan (option 4) is equally important, as it allows the infection preventionist to assess and update protocols—such as ventilation, personal protective equipment (PPE) use, and screening processes—to address the heightened risk posed by the growing number of cases among foreign-born individuals (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.2 - Implement measures to prevent transmission of infectious agents).
Option 2 (inform staff who are foreign-born) is not the best use of this data, as the information pertains to patient demographics rather than staff risk, and targeting staff based on their origin could be inappropriate without specific exposure evidence. Option 3 (educate patients and visitors) is a general education strategy but less directly actionable with this specific epidemiological data, which is more relevant to healthcare worker preparedness and facility protocols. Combining options 1 and 4 aligns with CBIC’s emphasis on using surveillance data to guide prevention and control measures, ensuring a proactive response to the increased TB burden (CBIC Practice Analysis, 2022, Domain II: Surveillance and Epidemiologic Investigation, Competency 2.5 - Use data to guide infection prevention and control strategies).
References: CBIC Practice Analysis, 2022, Domain II: Surveillance and Epidemiologic Investigation, Competencies 2.1 - Conduct surveillance for healthcare-associated infections and epidemiologically significant organisms, 2.5 - Use data to guide infection prevention and control strategies; Domain III: Infection Prevention and Control, Competency 3.2 - Implement measures to prevent transmission of infectious agents.
What is a characteristic of immediate-use steam sterilization?
Alternative to purchasing expensive instrument sets.
Can be used for the following surgery if properly stored.
Substitute for maintaining sufficient amounts of sterile instruments.
Performed in emergencies where cleaning is the most critical step.
The correct answer is C, "Substitute for maintaining sufficient amounts of sterile instruments," as this is a characteristic of immediate-use steam sterilization (IUSS). According to the Certification Board of Infection Control and Epidemiology (CBIC) guidelines, IUSS, formerly known as flash sterilization, is a process designed to rapidly sterilize items that are needed urgently when pre-sterilized inventory is unavailable or insufficient. It serves as a temporary solution to address gaps in sterile instrument availability, such as during unexpected surges in surgical demand or equipment shortages, provided strict protocols are followed (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.3 - Ensure safe reprocessing of medical equipment). However, IUSS is not a routine practice and should be minimized due to its limitations, including the lack of immediate biologic indicator results.
Option A (alternative to purchasing expensive instrument sets) is incorrect because IUSS is not intended as a cost-saving measure or a replacement for acquiring necessary equipment; it is a contingency process. Option B (can be used for the following surgery if properly stored) is misleading, as IUSS items are intended for immediate use and not for storage or use in subsequent procedures, which requires standard sterilization cycles with proper packaging and validation. Option D (performed in emergencies where cleaning is the most critical step) overemphasizes cleaning and mischaracterizes IUSS; while cleaning is a critical initial step, the process is defined by its rapid sterilization for emergency use, not solely by cleaning priority.
The characteristic of substituting for insufficient sterile instruments aligns with CBIC’s focus on ensuring safe reprocessing practices while acknowledging the practical challenges in healthcare settings (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.5 - Evaluate the environment for infection risks). This is supported by AAMI ST79, which outlines IUSS as a last-resort measure to maintain surgical readiness (AAMI ST79:2017).
References: CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competencies 3.3 - Ensure safe reprocessing of medical equipment, 3.5 - Evaluate the environment for infection risks. AAMI ST79:2017, Comprehensive guide to steam sterilization and sterility assurance in health care facilities.
Which of the following processes is essential for endoscope reprocessing?
Intermediate level disinfection and contact time
Pre-cleaning, leak testing, and manual cleaning
Inspection using a borescope and horizontal storage
Leak testing, manual cleaning, and low level disinfection
The correct answer is B, "Pre-cleaning, leak testing, and manual cleaning," as these processes are essential for endoscope reprocessing. According to the Certification Board of Infection Control and Epidemiology (CBIC) guidelines, proper reprocessing of endoscopes is critical to prevent healthcare-associated infections (HAIs), given their complex design and susceptibility to microbial contamination. The initial steps of pre-cleaning (removing gross debris at the point of use), leak testing (ensuring the endoscope’s integrity to prevent fluid ingress), and manual cleaning (using enzymatic detergents to remove organic material) are foundational to the reprocessing cycle. These steps prepare the endoscope for high-level disinfection or sterilization by reducing bioburden and preventing damage, as outlined in standards such as AAMI ST91 (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.3 - Ensure safe reprocessing of medical equipment). Failure at this stage can compromise subsequent disinfection, making it a non-negotiable component of the process.
Option A (intermediate level disinfection and contact time) is an important step but insufficient alone, as intermediate-level disinfection does not achieve the high-level disinfection required for semi-critical devices like endoscopes, which must eliminate all microorganisms except high levels of bacterial spores. Option C (inspection using a borescope and horizontal storage) includes valuable quality control (inspection) and storage practices, but these occur later in the process and are not essential initial steps; vertical storage is often preferred to prevent damage. Option D (leak testing, manual cleaning, and low level disinfection) includes two essential steps (leak testing and manual cleaning) but is inadequate because low-level disinfection does not meet the standard for endoscopes, which require high-level disinfection or sterilization.
The emphasis on pre-cleaning, leak testing, and manual cleaning aligns with CBIC’s focus on adhering to evidence-based reprocessing protocols to ensure patient safety and prevent HAIs (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.4 - Implement environmental cleaning and disinfection protocols). These steps are mandated by guidelines to mitigate risks associated with endoscope use in healthcare settings.
References: CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competencies 3.3 - Ensure safe reprocessing of medical equipment, 3.4 - Implement environmental cleaning and disinfection protocols. AAMI ST91:2015, Flexible and semi-rigid endoscope processing in health care facilities.
After defining and identifying cases in a possible cluster of infections, an infection preventionist should NEXT establish:
The route of transmission.
An appropriate control group.
A hypothesis that will explain the majority of cases.
Whether observed incidence exceeds expected incidence.
When investigating a possible cluster of infections, an infection preventionist (IP) follows a structured epidemiological approach to identify the cause and implement control measures. The Certification Board of Infection Control and Epidemiology (CBIC) outlines this process within the "Surveillance and Epidemiologic Investigation" domain, which aligns with the Centers for Disease Control and Prevention (CDC) guidelines for outbreak investigation. The steps typically include defining and identifying cases, formulating a hypothesis, testing the hypothesis, and implementing control measures. The question specifies the next step after defining and identifying cases, requiring an evaluation of the logical sequence.
Option C, "A hypothesis that will explain the majority of cases," is the next critical step. After confirming a cluster through case definition and identification (e.g., by time, place, and person), the IP should develop a working hypothesis to explain the observed pattern. This hypothesis might propose a common source (e.g., contaminated equipment), a mode of transmission (e.g., airborne), or a specific population at risk. The CDC’s "Principles of Epidemiology in Public Health Practice" (3rd Edition, 2012) emphasizes that formulating a hypothesis is essential to guide further investigation, such as identifying risk factors or environmental sources. This step allows the IP to focus resources on testing the most plausible explanation before proceeding to detailed analysis or interventions.
Option A, "The route of transmission," is an important element of the investigation but typically follows hypothesis formulation. Determining the route (e.g., contact, droplet, or common vehicle) requires data collection and analysis to test the hypothesis, making it a subsequent step rather than the immediate next action. Option B, "An appropriate control group," is relevant for analytical studies (e.g., case-control studies) to compare exposed versus unexposed individuals, but this is part of hypothesis testing, which occurs after the hypothesis is established. Selecting a control group prematurely, without a hypothesis, lacks direction and efficiency. Option D, "Whether observed incidence exceeds expected incidence," is a preliminary step to define a cluster, often done during case identification using baseline data or statistical thresholds (e.g., exceeding the mean plus two standard deviations). Since the question assumes cases are already defined and identified, this step is complete, and the focus shifts to hypothesis development.
The CBIC Practice Analysis (2022) and CDC guidelines prioritize hypothesis formulation as the logical next step after case identification, enabling a targeted investigation. This approach ensures that the IP can efficiently address the cluster’s cause, making Option C the correct answer.
References:
CBIC Practice Analysis, 2022.
CDC Principles of Epidemiology in Public Health Practice, 3rd Edition, 2012.
Immediate use steam sterilization is NOT recommended for implantable items requiring immediate use because
the high temperature may damage the items.
chemical indicators may not be accurate at high temperatures.
results of biologic indicators are unavailable prior to use of the item.
the length of time is inadequate for the steam to penetrate the pack.
The correct answer is C, "results of biologic indicators are unavailable prior to use of the item," as this is the primary reason immediate use steam sterilization (IUSS) is not recommended for implantable items requiring immediate use. According to the Certification Board of Infection Control and Epidemiology (CBIC) guidelines, IUSS is a process used for sterilizing items needed urgently when no other sterile options are available, typically involving a shortened cycle (e.g., flash sterilization). However, for implantable items—such as orthopedic hardware or prosthetic devices—ensuring absolute sterility is critical due to the risk of deep infection. Biologic indicators (BIs), which contain highly resistant spores to verify sterilization efficacy, require incubation (typically 24-48 hours) to confirm the kill, but IUSS does not allow time for BI results to be available before the item is used (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.3 - Ensure safe reprocessing of medical equipment). This lack of immediate verification poses a significant infection risk, making IUSS inappropriate for implants, as per AAMI ST79 standards.
Option A (the high temperature may damage the items) is a consideration for some heat-sensitive materials, but modern IUSS cycles are designed to minimize damage, and this is not the primary reason for the restriction on implants. Option B (chemical indicators may not be accurate at high temperatures) is incorrect, as chemical indicators (e.g., color-changing strips) are reliable at high temperatures and serve as an immediate check, though they are not a substitute for BIs. Option D (the length of time is inadequate for the steam to penetrate the pack) is not the main issue, as IUSS cycles are optimized for penetration, though the shortened time may be a secondary concern; the unavailability of BI results remains the decisive factor.
The focus on biologic indicator results aligns with CBIC’s emphasis on ensuring the safety and sterility of reprocessed medical devices, particularly for high-risk implantable items (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.5 - Evaluate the environment for infection risks). This recommendation is supported by AAMI and CDC guidelines, which prioritize BI confirmation for implants to prevent healthcare-associated infections (AAMI ST79:2017, CDC Sterilization Guidelines, 2019).
References: CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competencies 3.3 - Ensure safe reprocessing of medical equipment, 3.5 - Evaluate the environment for infection risks. AAMI ST79:2017, Comprehensive guide to steam sterilization and sterility assurance in health care facilities. CDC Guidelines for Disinfection and Sterilization in Healthcare Facilities, 2019.
Given the formula for calculating incidence rates, the Y represents which of the following?

Population served
Number of infected patients
Population at risk
Number of events
Incidence rate is a fundamental epidemiological measure used to quantify the frequency of new cases of a disease within a specified population over a defined time period. The Certification Board of Infection Control and Epidemiology (CBIC) supports the use of such metrics in the "Surveillance and Epidemiologic Investigation" domain, aligning with the Centers for Disease Control and Prevention (CDC) "Principles of Epidemiology in Public Health Practice" (3rd Edition, 2012). The formula provided, XY×K=Rate\frac{X}{Y} \times K = RateYX×K=Rate, represents the standard incidence rate calculation, where KKK is a constant (e.g., 1,000 or 100,000) to express the rate per unit population, and the question asks what YYY represents among the given options.
In the incidence rate formula, XXX typically represents the number of new cases (or events) of the disease occurring during a specific period, and YYY represents the population at risk during that same period. The ratio XY\frac{X}{Y}YX yields the rate per unit of population, which is then multiplied by KKK to standardize the rate (e.g., cases per 1,000 persons). The CDC defines the denominator (YYY) as the population at risk, which includes individuals susceptible to the disease over the observation period. Option B ("Number of infected patients") might suggest XXX if it specified new cases, but as the denominator YYY, it is incorrect because incidence focuses on new cases relative to the at-risk population, not the total number of infected individuals (which could include prevalent cases). Option C ("Population at risk") correctly aligns with YYY, representing the base population over which the rate is calculated.
Option A, "Population served," is a broader term that might include the total population under care (e.g., in a healthcare facility), but it is not specific to those at risk for new infections, making it less precise. Option D, "Number of events," could align with XXX (new cases or events), but as the denominator YYY, it does not fit the formula’s structure. The CBIC Practice Analysis (2022) and CDC guidelines reinforce that the denominator in incidence rates is the population at risk, ensuring accurate measurement of new disease occurrence.
References:
CBIC Practice Analysis, 2022.
CDC Principles of Epidemiology in Public Health Practice, 3rd Edition, 2012.
A 17-year-old presents to the Emergency Department with fever, stiff neck, and vomiting. A lumbar puncture is done. The Gram stain shows Gram negative diplocooci. Presumptive identification of the organism is
Haemophilus influenzae
Neisseria meningitidis
Listeria monocytogenes
Streptococcus pneumoniae
The Gram stain showing Gram-negative diplococci in cerebrospinal fluid (CSF) is characteristic of Neisseria meningitidis, a leading cause of bacterial meningitis in adolescents and young adults.
Step-by-Step Justification:
Gram Stain Interpretation:
Gram-negative diplococci in CSF strongly suggest Neisseria meningitidis.
Classic Symptoms of Meningitis:
Fever, stiff neck, and vomiting are hallmark signs of meningococcal meningitis.
Neisseria meningitidis vs. Other Bacteria:
Haemophilus influenzae (Option A) → Gram-negative coccobacilli.
Listeria monocytogenes (Option C) → Gram-positive rods.
Streptococcus pneumoniae (Option D) → Gram-positive diplococci.
CBIC Infection Control References:
APIC Ready Reference for Microbes, "Neisseria meningitidis and Meningitis".
Therapeutic antimicrobial agents should be used when
the infecting agent is unknown
the patient's illness warrants treatment prior to culture results
the patient symptoms suggest likely pathogens.
Following identification of the pathogen and sensitives.
Therapeutic antimicrobial agents should ideally be pathogen-directed to minimize resistance, side effects, and treatment failure. Once the causative pathogen and its antimicrobial susceptibilities are known, the most narrow-spectrum, effective agent should be used.
Why the Other Options Are Incorrect?
A. The infecting agent is unknown – Empiric therapy may be necessary initially, but definitive therapy should be based on pathogen identification.
B. The patient's illness warrants treatment prior to culture results – This applies to empiric therapy, but not to definitive antimicrobial selection.
C. The patient’s symptoms suggest likely pathogens – Clinical presentation guides empiric treatment, but definitive therapy should follow culture and susceptibility testing.
CBIC Infection Control Reference
APIC emphasizes the importance of selecting antimicrobials based on pathogen identification and susceptibility testing to prevent antimicrobial resistance.
Surgical site infection (SSI) data for the previous quarter reveal the following numbers. The surgeon with the highest infection rate is Doctor
Brown
Jones.
Smith
White
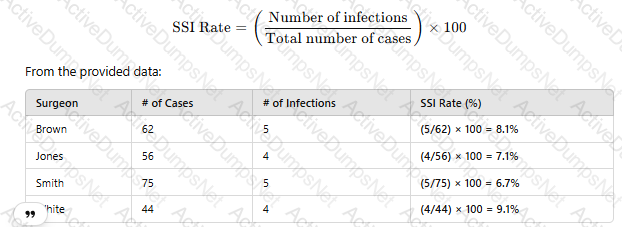
To determine which surgeon has the highest surgical site infection (SSI) rate, use the following formula:
 A screenshot of a report
AI-generated content may be incorrect.
A screenshot of a report
AI-generated content may be incorrect.
Since Dr. White has the highest SSI rate at 9.1%, the correct answer is D. White.
CBIC Infection Control Reference
SSI rates are calculated using infection count per total procedures and reported as percentage values.
During the last week in June, an emergency department log reveals numerous cases of profuse watery diarrhea in individuals 74 years of age and older. During the same time period, four immunocompromised patients were admitted with possible Cryptosporidium. Which of the following actions should the infection preventionist take FIKST?
Characterize the outbreak by person, place, and time
Increase surveillance facility wide for additional cases
Contact the laboratory to confirm stool identification results
Form a tentative hypothesis about the potential reservoir for this outbreak
When an outbreak of infectious disease is suspected, the first step is to conduct an epidemiologic investigation. This begins with characterizing the outbreak by person, place, and time to establish patterns and trends. This approach, known as descriptive epidemiology, provides critical insights into potential sources and transmission patterns.
Step-by-Step Justification:
Identify Cases and Patterns:
The infection preventionist should analyze patient demographics (person), locations of cases (place), and onset of symptoms (time). This helps in defining the outbreak scope and potential exposure sources.
Create an Epidemic Curve:
An epidemic curve helps determine whether the outbreak is a point-source or propagated event. This can indicate whether the infection is spreading person-to-person or originating from a common source.
Compare with Baseline Data:
Reviewing historical data ensures that the observed cases exceed the expected norm, confirming an outbreak.
Guide Further Investigation:
Establishing basic epidemiologic patterns guides subsequent actions, such as laboratory testing, environmental sampling, and surveillance.
Why Other Options Are Incorrect:
B. Increase surveillance facility-wide for additional cases:
While enhanced surveillance is important, it should follow the initial characterization of the outbreak. Surveillance without a defined case profile may lead to misclassification and misinterpretation.
C. Contact the laboratory to confirm stool identification results:
Confirming lab results is essential but comes after defining the outbreak's characteristics. Without an epidemiologic link, testing may yield results that are difficult to interpret.
D. Form a tentative hypothesis about the potential reservoir for this outbreak:
Hypothesis generation occurs after sufficient epidemiologic data have been collected. Jumping to conclusions without characterization may result in incorrect assumptions and ineffective control measures.
CBIC Infection Control References:
APIC Text, "Outbreak Investigations," Epidemiology, Surveillance, Performance, and Patient Safety Measures.
APIC/JCR Infection Prevention and Control Workbook, Chapter 4, Surveillance Program.
APIC Text, "Investigating Infectious Disease Outbreaks," Guidelines for Epidemic Curve Analysis.
Hand hygiene rates in the facility have been decreasing over time. The Infection Preventionist (IP) surveys staff and finds that hand dryness is the major reason for non-compliance. What step should the IP take?
Provide staff lotion in every patient room.
Provide a compatible lotion in a convenient location.
Allow staff to bring in lotion and carry it in their pockets.
Allow staff to bring in lotion for use at the nurses’ station and lounge.
Hand hygiene is a cornerstone of infection prevention, and declining compliance rates pose a significant risk for healthcare-associated infections (HAIs). The Certification Board of Infection Control and Epidemiology (CBIC) emphasizes improving hand hygiene adherence in the "Prevention and Control of Infectious Diseases" domain, aligning with the Centers for Disease Control and Prevention (CDC) "Guideline for Hand Hygiene in Healthcare Settings" (2002). The IP’s survey identifies hand dryness as the primary barrier, likely due to the frequent use of alcohol-based hand sanitizers or soap, which can dehydrate skin. The goal is to address this barrier effectively while maintaining infection control standards.
Option B, "Provide a compatible lotion in a convenient location," is the most appropriate step. The CDC and World Health Organization (WHO) recommend using moisturizers to mitigate skin irritation and dryness, which can improve hand hygiene compliance. However, the lotion must be compatible with alcohol-based hand rubs (e.g., free of petroleum-based products that can reduce sanitizer efficacy) and placed in accessible areas (e.g., near sinks or sanitizer dispensers) to encourage use without disrupting workflow. The WHO’s "Guidelines on Hand Hygiene in Health Care" (2009) suggest providing skin care products as part of a multimodal strategy to enhance adherence, making this a proactive, facility-supported solution that addresses the root cause.
Option A, "Provide staff lotion in every patient room," is a good intention but impractical and potentially risky. Placing lotion in patient rooms could lead to inconsistent use, contamination (e.g., from patient contact), or misuse (e.g., staff applying incompatible products), compromising infection control. The CDC advises against uncontrolled lotion distribution in patient care areas. Option C, "Allow staff to bring in lotion and carry it in their pockets," introduces variability in product quality and compatibility. Personal lotions may contain ingredients (e.g., oils) that inactivate alcohol-based sanitizers, and pocket storage increases the risk of contamination or cross-contamination, which the CDC cautions against. Option D, "Allow staff to bring in lotion for use at the nurses’ station and lounge," limits the intervention to non-patient care areas, reducing its impact on hand hygiene during patient interactions. It also shares the compatibility and contamination risks of Option C, making it less effective.
The CBIC Practice Analysis (2022) and CDC guidelines emphasize evidence-based interventions, such as providing approved skin care products in strategic locations to boost compliance. Option B balances accessibility, safety, and compatibility, making it the best step to address hand dryness and improve hand hygiene rates.
References:
CBIC Practice Analysis, 2022.
CDC Guideline for Hand Hygiene in Healthcare Settings, 2002.
WHO Guidelines on Hand Hygiene in Health Care, 2009.
A healthcare personnel has an acute group A streptococcal throat infection. What is the earliest recommended time that this person may return to work after receiving appropriate antibiotic therapy?
8 hours
24 hours
48 hours
72 hours
The correct answer is B, "24 hours," as this is the earliest recommended time that a healthcare personnel with an acute group A streptococcal throat infection may return to work after receiving appropriate antibiotic therapy. According to the Certification Board of Infection Control and Epidemiology (CBIC) guidelines, which align with recommendations from the Centers for Disease Control and Prevention (CDC), healthcare workers with group A Streptococcus (GAS) infections, such as streptococcal pharyngitis, should be treated with antibiotics (e.g., penicillin or a suitable alternative) to eradicate the infection and reduce transmission risk. The CDC and Occupational Safety and Health Administration (OSHA) guidelines specify that healthcare personnel can return to work after at least 24 hours of effective antibiotic therapy, provided they are afebrile and symptoms are improving, as this period is sufficient to significantly reduce the bacterial load and contagiousness (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.2 - Implement measures to prevent transmission of infectious agents).
Option A (8 hours) is too short a duration to ensure the infection is adequately controlled and the individual is no longer contagious. Option C (48 hours) and Option D (72 hours) are longer periods that may apply in some cases (e.g., if symptoms persist or in outbreak settings), but they exceed the minimum recommended time based on current evidence. The 24-hour threshold is supported by studies showing that GAS shedding decreases substantially within this timeframe with appropriate antibiotic treatment, minimizing the risk to patients and colleagues (CDC Guidelines for Infection Control in Healthcare Personnel, 2019).
The infection preventionist’s role includes enforcing return-to-work policies to prevent healthcare-associated infections (HAIs), aligning with CBIC’s emphasis on timely and evidence-based interventions to control infectious disease transmission in healthcare settings (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.1 - Collaborate with organizational leaders). Compliance with this recommendation also supports occupational health protocols to balance staff safety and patient care.
References: CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competencies 3.1 - Collaborate with organizational leaders, 3.2 - Implement measures to prevent transmission of infectious agents. CDC Guidelines for Infection Control in Healthcare Personnel, 2019.
Peripherally inserted central catheter (PICC)-associated bloodstream infections (BSIs) have been increasing over the past four months. Which of the following interventions is MOST likely to have contributed to the increase?
Use of chlorhexidine skin antisepsis during insertion of the PICC
Daily bathing adult intensive care unit patients with chlorhexidine
Replacement of the intravenous administration sets every 72 hours
Use of a positive pressure device on the PICC
Peripherally inserted central catheter (PICC)-associated bloodstream infections (BSIs) are a significant concern in healthcare settings, and identifying factors contributing to their increase is critical for infection prevention. The Certification Board of Infection Control and Epidemiology (CBIC) emphasizes the "Surveillance and Epidemiologic Investigation" and "Prevention and Control of Infectious Diseases" domains, which align with the Centers for Disease Control and Prevention (CDC) guidelines for preventing intravascular catheter-related infections. The question asks for the intervention most likely to have contributed to the rise in PICC-associated BSIs over four months, requiring an evaluation of each option based on evidence-based practices.
Option C, "Replacement of the intravenous administration sets every 72 hours," is the most likely contributor to the increase. The CDC’s "Guidelines for the Prevention of Intravascular Catheter-Related Infections" (2017) recommend that intravenous administration sets (e.g., tubing for fluids or medications) be replaced no more frequently than every 72-96 hours unless clinically indicated (e.g., contamination or specific therapy requirements). Frequent replacement, such as every 72 hours as a routine practice, can introduce opportunities for contamination during the change process, especially if aseptic technique is not strictly followed. Studies cited in the CDC guidelines, including those by O’Grady et al. (2011), indicate that unnecessary manipulation of catheter systems increases the risk of introducing pathogens, potentially leading to BSIs. A change to a 72-hour replacement schedule, if not previously standard, could explain the observed increase over the past four months.
Option A, "Use of chlorhexidine skin antisepsis during insertion of the PICC," is a recommended practice to reduce BSIs. Chlorhexidine, particularly in a 2% chlorhexidine gluconate with 70% alcohol solution, is the preferred skin antiseptic for catheter insertion due to its broad-spectrum activity and residual effect, as supported by the CDC (2017). This intervention should decrease, not increase, infection rates, making it an unlikely contributor. Option B, "Daily bathing adult intensive care unit patients with chlorhexidine," is another evidence-based strategy to reduce healthcare-associated infections, including BSIs, by decolonizing the skin of pathogens like Staphylococcus aureus. The CDC and SHEA (Society for Healthcare Epidemiology of America) guidelines (2014) endorse chlorhexidine bathing in intensive care units, suggesting it should lower, not raise, BSI rates. Option D, "Use of a positive pressure device on the PICC," aims to prevent catheter occlusion and reduce the need for frequent flushing, which could theoretically decrease infection risk by minimizing manipulation. However, there is no strong evidence linking positive pressure devices to increased BSIs; if improperly used or maintained, they might contribute marginally, but this is less likely than the impact of frequent tubing changes.
The CBIC Practice Analysis (2022) and CDC guidelines highlight that deviations from optimal catheter maintenance practices, such as overly frequent administration set replacements, can increase infection risk. Given the four-month timeframe and the focus on an intervention’s potential negative impact, Option C stands out as the most plausible contributor due to the increased manipulation and contamination risk associated with routine 72-hour replacements.
References:
CBIC Practice Analysis, 2022.
CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2017.
O’Grady, N. P., et al. (2011). Guidelines for the Prevention of Intravascular Catheter-Related Infections. Clinical Infectious Diseases.
SHEA Compendium, Strategies to Prevent Central Line-Associated Bloodstream Infections, 2014.
Which of the following patients with human immunodeficiency virus infection requires Airborne precautions?
24-year-old male newly diagnosed with a CD4 count of 70
28-year-old female with Mycobacterium avium in sputum
36-year-old male with cryptococcal meningitis
46-year-old female with a cavitary lesion in upper lobe
HIV patients require Airborne Precautions if they have tuberculosis (TB). A cavitary lesion in the upper lobe is highly suggestive of active pulmonary TB, which requires Airborne Precautions due to aerosolized transmission.
Why the Other Options Are Incorrect?
A. 24-year-old male newly diagnosed with a CD4 count of 70 – Low CD4 count alone does not warrant Airborne Precautions unless there is active TB or another airborne pathogen.
B. 28-year-old female with Mycobacterium avium in sputum – Mycobacterium avium complex (MAC) is not airborne, and standard precautions are sufficient.
C. 36-year-old male with cryptococcal meningitis – Cryptococcus neoformans is not transmitted via the airborne route, so Airborne Precautions are unnecessary.
CBIC Infection Control Reference
Patients with HIV and suspected TB require Airborne Precautions until TB is ruled out.
An employee is presenting to Occupational Health for clearance prior to starting work at a healthcare facility. They have a history of having received the Bacillus Calmette-Guérin (BCG) vaccination. What is the preferred methodology for pre-work clearance?
Referral to tuberculosis (TB) clinic
Initial chest radiograph
Interferon-gamma release assay
Two-step purified protein derivative-based Tuberculin skin test (TST)
The preferred methodology for pre-work clearance in this scenario is the interferon-gamma release assay (IGRA), making option C the correct choice. This conclusion is supported by the guidelines from the Certification Board of Infection Control and Epidemiology (CBIC), which align with recommendations from the Centers for Disease Control and Prevention (CDC) for tuberculosis (TB) screening in healthcare workers. The employee’s history of receiving the Bacillus Calmette-Guérin (BCG) vaccination, a vaccine commonly used in some countries to prevent severe forms of TB, is significant because it can cause false-positive results in the traditional Tuberculin skin test (TST) due to cross-reactivity with BCG antigens (CBIC Practice Analysis, 2022, Domain I: Identification of Infectious Disease Processes, Competency 1.3 - Apply principles of epidemiology).
The IGRA, such as the QuantiFERON-TB Gold test, measures the release of interferon-gamma from T-cells in response to specific TB antigens (e.g., ESAT-6 and CFP-10) that are not present in BCG or most non-tuberculous mycobacteria. This makes it a more specific and reliable test for detecting latent TB infection (LTBI) in individuals with a history of BCG vaccination, avoiding the false positives associated with the TST. The CDC recommends IGRA over TST for BCG-vaccinated individuals when screening for TB prior to healthcare employment (CDC Guidelines for Preventing Transmission of Mycobacterium tuberculosis, 2005, updated 2019).
Option A (referral to tuberculosis clinic) is a general action but not a specific methodology for clearance; it may follow testing if results indicate further evaluation is needed. Option B (initial chest radiograph) is used to detect active TB disease rather than latent infection and is not a primary screening method for pre-work clearance, though it may be indicated if IGRA results are positive. Option D (two-step purified protein derivative-based Tuberculin skin test) is less preferred because the BCG vaccination can lead to persistent cross-reactivity, reducing its specificity and reliability in this context. The two-step TST is typically used to establish a baseline in unvaccinated individuals with potential prior exposure, but it is not ideal for BCG-vaccinated individuals.
The IP’s role includes ensuring accurate TB screening to protect both the employee and patients, aligning with CBIC’s focus on preventing transmission of infectious diseases in healthcare settings (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.2 - Implement measures to prevent transmission of infectious agents).
References: CBIC Practice Analysis, 2022, Domain I: Identification of Infectious Disease Processes, Competency 1.3 - Apply principles of epidemiology; Domain III: Infection Prevention and Control, Competency 3.2 - Implement measures to prevent transmission of infectious agents. CDC Guidelines for Preventing Transmission of Mycobacterium tuberculosis, 2005, updated 2019.
A hospital is experiencing an increase in multidrug-resistant Acinetobacter baumannii infections in the intensive care unit (ICU). The infection preventionist's FIRST action should be to:
Implement universal contact precautions for all ICU patients.
Conduct an epidemiologic investigation to identify potential sources.
Perform environmental sampling to detect Acinetobacter on surfaces.
Initiate decolonization protocols for all ICU patients.
Epidemiologic Investigation:
The first step in an outbreak response is to characterize cases by person, place, and time.
Identifying common exposures (e.g., ventilators, catheters, or contaminated surfaces) helps determine the source.
Why Other Options Are Incorrect:
A. Universal contact precautions: Premature; precautions should be tailored based on transmission patterns.
C. Environmental sampling: Should be done after identifying epidemiologic links.
D. Decolonization protocols: Not routinely recommended for Acinetobacter outbreaks.
CBIC Infection Control References:
CIC Study Guide, "Epidemiologic Investigations in Outbreaks," Chapter 4.
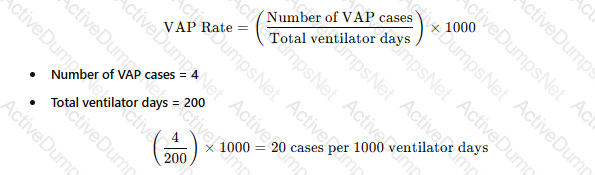
There are four cases of ventilator-associated pneumonia in a surgical intensive care unit with a total of 200 ventilator days and a census of 12 patients. Which of the following BEST expresses how this should be reported?
Ventilator-associated pneumonia rate of 2%
20 ventilator-associated pneumonia cases/1000 ventilator days
Postoperative pneumonia rate of 6% in SICU patients
More information is needed regarding ventilator days per patient
The standard way to report ventilator-associated pneumonia (VAP) rates is:
 A white paper with black text
AI-generated content may be incorrect.
A white paper with black text
AI-generated content may be incorrect.
Why the Other Options Are Incorrect?
A. Ventilator-associated pneumonia rate of 2% – This does not use the correct denominator (ventilator days).
C. Postoperative pneumonia rate of 6% in SICU patients – Not relevant, as the data focuses on VAP, not postoperative pneumonia.
D. More information is needed regarding ventilator days per patient – The total ventilator days are already provided, so no additional data is required.
CBIC Infection Control Reference
APIC and NHSN recommend reporting VAP rates as cases per 1,000 ventilator days.
Which statistical test is MOST appropriate for comparing infection rates before and after an intervention?
Student’s t-test
Chi-square test for proportions
Linear regression analysis
Wilcoxon rank-sum test
The Chi-square test is the most appropriate test for comparing infection rates (categorical data) before and after an intervention.
CBIC Infection Control References:
CIC Study Guide, "Statistical Analysis in Infection Control," Chapter 5.
An infection preventionist (IP) is tasked with developing an infection prevention training program for family members. What step should the IP take FIRST?
Assess the needs of the family members at the facility.
Create clearly defined goals and objectives for the training.
Ensure that all content in the training is relevant and practical.
Develop a plan to create an appropriate training environment.
The correct answer is A, "Assess the needs of the family members at the facility," as this is the first step the infection preventionist (IP) should take when developing an infection prevention training program for family members. According to the Certification Board of Infection Control and Epidemiology (CBIC) guidelines, effective education programs begin with a needs assessment to identify the specific knowledge gaps, cultural factors, and practical challenges of the target audience—in this case, family members. This initial step ensures that the training is tailored to their level of understanding, language preferences, and the infection risks they may encounter (e.g., hand hygiene, isolation protocols), aligning with adult learning principles (CBIC Practice Analysis, 2022, Domain IV: Education and Research, Competency 4.1 - Develop and implement educational programs). Without this assessment, subsequent steps risk being misaligned with the audience’s needs, reducing the program’s effectiveness.
Option B (create clearly defined goals and objectives for the training) is a critical step but follows the needs assessment, as goals should be based on identified needs to ensure relevance. Option C (ensure that all content in the training is relevant and practical) depends on understanding the audience’s needs first, making it a later step in the development process. Option D (develop a plan to create an appropriate training environment) is important for implementation but requires prior knowledge of the audience and content to design effectively.
The focus on assessing needs aligns with CBIC’s emphasis on evidence-based education design, enabling the IP to address specific infection prevention priorities for family members and improve outcomes in the facility (CBIC Practice Analysis, 2022, Domain IV: Education and Research, Competency 4.2 - Evaluate the effectiveness of educational programs). This approach is supported by CDC guidelines, which recommend audience assessment as a foundational step in health education programs.
References: CBIC Practice Analysis, 2022, Domain IV: Education and Research, Competencies 4.1 - Develop and implement educational programs, 4.2 - Evaluate the effectiveness of educational programs. CDC Health Education Curriculum Analysis Tool, 2019.
An infection preventionist (IP) encounters a surgeon at the nurse’s station who loudly disagrees with the IP’s surgical site infection findings. The IP’s BEST response is to:
Report the surgeon to the chief of staff.
Calmly explain that the findings are credible.
Ask the surgeon to speak in a more private setting to review their concerns.
Ask the surgeon to change their tone and leave the nurses’ station if they refuse.
The scenario involves a conflict between an infection preventionist (IP) and a surgeon regarding surgical site infection (SSI) findings, occurring in a public setting (the nurse’s station). The IP’s response must align with professional communication standards, infection control priorities, and the principles of collaboration and conflict resolution as emphasized by the Certification Board of Infection Control and Epidemiology (CBIC). The “best” response should de-escalate the situation, maintain professionalism, and facilitate a constructive dialogue. Let’s evaluate each option:
A. Report the surgeon to the chief of staff: Reporting the surgeon to the chief of staff might be considered if the behavior escalates or violates policy (e.g., harassment or disruption), but it is an escalation that should be a last resort. This action does not address the immediate disagreement about the SSI findings or attempt to resolve the issue collaboratively. It could also strain professional relationships and is not the best initial response, as it bypasses direct communication.
B. Calmly explain that the findings are credible: Explaining the credibility of the findings is important and demonstrates the IP’s confidence in their work, which is based on evidence-based infection control practices. However, doing so in a public setting like the nurse’s station, especially with a loud disagreement, may not be effective. The surgeon may feel challenged or defensive, potentially worsening the situation. While this response has merit, it lacks consideration of the setting and the need for privacy to discuss sensitive data.
C. Ask the surgeon to speak in a more private setting to review their concerns: This response is the most appropriate as it addresses the immediate need to de-escalate the public confrontation and move the discussion to a private setting. It shows respect for the surgeon’s concerns, maintains professionalism, and allows the IP to review the SSI findings (e.g., data collection methods, definitions, or surveillance techniques) in a controlled environment. This aligns with CBIC’s emphasis on effective communication and collaboration with healthcare teams, as well as the need to protect patient confidentiality and maintain a professional atmosphere. It also provides an opportunity to educate the surgeon on the evidence behind the findings, which is a key IP role.
D. Ask the surgeon to change their tone and leave the nurses’ station if they refuse: Requesting a change in tone is reasonable given the loud disagreement, but demanding the surgeon leave if they refuse is confrontational and risks escalating the conflict. This approach could damage the working relationship and does not address the underlying disagreement about the SSI findings. While maintaining a respectful environment is important, this response prioritizes control over collaboration and is less constructive than seeking a private discussion.
The best response is C, as it promotes a professional, collaborative approach by moving the conversation to a private setting. This allows the IP to address the surgeon’s concerns, explain the SSI surveillance methodology (e.g., NHSN definitions or CBIC guidelines), and maintain a positive working relationship, which is critical for effective infection prevention programs. This strategy reflects CBIC’s focus on leadership, communication, and teamwork in healthcare settings.
References:
CBIC Infection Prevention and Control (IPC) Core Competency Model (updated 2023), Domain V: Management and Communication, which stresses effective interpersonal communication and conflict resolution.
CBIC Examination Content Outline, Domain V: Leadership and Program Management, which includes collaborating with healthcare personnel and addressing disagreements professionally.
CDC Guidelines for SSI Surveillance (2023), which emphasize the importance of clear communication of findings to healthcare teams.
The Environmental Services department is purchasing a new disinfectant that is an approved hospital disinfectant with no tuberculocidal claim. This product is appropriate for cleaning which of the following items?
Laryngoscope blades
Blood pressure cuff
Respiratory therapy equipment
Ultrasound probe
Which of the following is the BEST strategy for reducing bloodstream infections associated with central venous catheters?
Routine replacement of central lines every 7 days.
Use of chlorhexidine-impregnated dressings.
Daily blood cultures for patients with central lines.
Use of povidone-iodine instead of chlorhexidine for skin antisepsis.
Chlorhexidine-impregnated dressings reduce central line-associated bloodstream infections (CLABSI) by preventing bacterial colonization.
Routine catheter replacement (A) increases insertion risks without reducing infections.
Daily blood cultures (C) are unnecessary and lead to false positives.
Povidone-iodine (D) is less effective than chlorhexidine for skin antisepsis.
CBIC Infection Control References:
APIC Text, "CLABSI Prevention Measures," Chapter 10.
An infection control manager is training a new infection preventionist. In discussing surveillance strategies, which of the following types of hospital infection surveillance usually provides maximum benefit with minimum resources?
High-risk patient focus
Antibiotic monitoring
Prevalence surveys
Nursing care plan review
A high-risk patient focus maximizes benefits while minimizing resource use in infection surveillance.
Step-by-Step Justification:
Efficiency of High-Risk Surveillance:
Targeting ICU, immunocompromised patients, or surgical units helps detect infections where the risk is highest, leading to earlier interventions.
Resource Allocation:
Full hospital-wide surveillance is resource-intensive; focusing on high-risk groups is more efficient.
Why Other Options Are Incorrect:
B. Antibiotic monitoring:
Important for stewardship, but not the primary focus of infection surveillance.
C. Prevalence surveys:
Snapshot data only; does not provide ongoing monitoring.
D. Nursing care plan review:
Less direct in identifying infection trends.
CBIC Infection Control References:
APIC Text, "Surveillance Strategies for Infection Prevention".
In which of the following ways is human immunodeficiency virus similar to the Hepatitis B virus?
The primary mechanism of transmission for both is maternal-fetal
Needlestick exposure leads to a high frequency of healthcare worker infection
Transmission may occur from asymptomatic carriers
The risk of infection from mucous membrane exposure is the same
The human immunodeficiency virus (HIV) and Hepatitis B virus (HBV) are both bloodborne pathogens that pose significant risks in healthcare settings, and understanding their similarities is crucial for infection prevention and control. The Certification Board of Infection Control and Epidemiology (CBIC) emphasizes the importance of recognizing transmission modes and implementing appropriate precautions in the "Prevention and Control of Infectious Diseases" domain, aligning with guidelines from the Centers for Disease Control and Prevention (CDC). Comparing these viruses involves evaluating their epidemiology, transmission routes, and occupational risks.
Option C, "Transmission may occur from asymptomatic carriers," is the correct answer. Both HIV and HBV can be transmitted by individuals who are infected but show no symptoms, making asymptomatic carriage a significant similarity. For HBV, chronic carriers (estimated at 257 million globally per WHO, 2019) can transmit the virus through blood, semen, or other bodily fluids without overt signs of disease. Similarly, HIV-infected individuals can remain asymptomatic for years during the latent phase, yet still transmit the virus through sexual contact, blood exposure, or perinatal transmission. The CDC’s "Guidelines for Prevention of Transmission of HIV and HBV to Healthcare Workers" (1987, updated 2011) and "Epidemiology and Prevention of Viral Hepatitis" (2018) highlight this shared characteristic, underscoring the need for universal precautions regardless of symptom status.
Option A, "The primary mechanism of transmission for both is maternal-fetal," is incorrect. While maternal-fetal transmission (perinatal transmission) is a significant route for both HIV and HBV—occurring in 5-10% of cases without intervention for HBV and 15-45% for HIV without antiretroviral therapy—it is not the primary mechanism. For HBV, the primary mode is horizontal transmission through unprotected sexual contact or percutaneous exposure (e.g., needlesticks), accounting for the majority of cases. For HIV, sexual transmission and intravenous drug use are the leading modes globally, with maternal-fetal transmission being a smaller proportion despite its importance. Option B, "Needlestick exposure leads to a high frequency of healthcare worker infection," is partially true but not a precise similarity. Needlestick exposures carry a high risk for HBV (transmission risk ~30% if the source is HBeAg-positive) and a lower risk for HIV (~0.3%), but the frequency of infection among healthcare workers is significantly higher for HBV due to its greater infectivity and stability outside the host. This makes the statement more characteristic of HBV than a shared trait. Option D, "The risk of infection from mucous membrane exposure is the same," is false. The risk of HIV transmission via mucous membrane exposure (e.g., splash to eyes or mouth) is approximately 0.09%, while for HBV it is higher (up to 1-2% depending on viral load and exposure type), reflecting HBV’s greater infectivity.
The CBIC Practice Analysis (2022) and CDC guidelines emphasize the role of asymptomatic transmission in shaping infection control strategies, such as routine testing and post-exposure prophylaxis. This shared feature of HIV and HBV justifies Option C as the most accurate similarity.
References:
CBIC Practice Analysis, 2022.
CDC Guidelines for Prevention of Transmission of HIV and HBV to Healthcare Workers, 2011.
CDC Epidemiology and Prevention of Viral Hepatitis, 2018.
WHO Hepatitis B Fact Sheet, 2019.
Each item or package that is prepared for sterilization should be labeled with the
storage location.
type of sterilization process.
sterilizer identification number or code.
cleaning method (e.g., mechanical or manual).
The correct answer is C, "sterilizer identification number or code," as this is the essential information that each item or package prepared for sterilization should be labeled with. According to the Certification Board of Infection Control and Epidemiology (CBIC) guidelines, proper labeling of sterilized items is a critical component of infection prevention and control to ensure traceability and verify the sterilization process. The sterilizer identification number or code links the item to a specific sterilization cycle, allowing the infection preventionist (IP) and sterile processing staff to track the equipment used, confirm compliance with standards (e.g., AAMI ST79), and facilitate recall or investigation if issues arise (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.3 - Ensure safe reprocessing of medical equipment). This labeling ensures that the sterility of the item can be assured and documented, protecting patient safety by preventing the use of inadequately processed items.
Option A (storage location) is important for inventory management but is not directly related to the sterilization process itself and does not provide evidence of the sterilization event. Option B (type of sterilization process) indicates the method (e.g., steam, ethylene oxide), which is useful but less critical than the sterilizer identification, as the process type alone does not confirm the specific cycle or equipment used. Option D (cleaning method, e.g., mechanical or manual) is a preliminary step in reprocessing, but it is not required on the sterilization label, as the focus shifts to sterilization verification once the item is prepared.
The requirement for a sterilizer identification number or code aligns with CBIC’s emphasis on maintaining rigorous tracking and quality assurance in the reprocessing of medical devices, ensuring accountability and adherence to best practices (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.5 - Evaluate the environment for infection risks). This practice is mandated by standards such as AAMI ST79 to support effective infection control in healthcare settings.
References: CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competencies 3.3 - Ensure safe reprocessing of medical equipment, 3.5 - Evaluate the environment for infection risks. AAMI ST79:2017, Comprehensive guide to steam sterilization and sterility assurance in health care facilities.
Which of the following activities will BEST prepare a newly hired infection preventionist to present information at the facility’s orientation program?
Observing other departments’ orientation presentations
Meeting with the facility’s leadership
Reviewing principles of adult learning
Administering tuberculin skin tests to orientees
The correct answer is C, "Reviewing principles of adult learning," as this activity will best prepare a newly hired infection preventionist to present information at the facility’s orientation program. According to the Certification Board of Infection Control and Epidemiology (CBIC) guidelines, effective education delivery, especially for healthcare professionals during orientation, relies on understanding adult learning principles (e.g., andragogy), which emphasize learner-centered approaches, relevance to practice, and active participation. Reviewing these principles equips the infection preventionist (IP) to design and deliver content that addresses the specific needs, experiences, and motivations of the audience—such as new staff learning infection control protocols—enhancing engagement and retention (CBIC Practice Analysis, 2022, Domain IV: Education and Research, Competency 4.1 - Develop and implement educational programs). This preparation ensures the presentation is tailored, impactful, and aligned with the goal of promoting infection prevention behaviors.
Option A (observing other departments’ orientation presentations) can provide insights into presentation styles or facility norms, but it is less focused on the IP’s specific educational role and may not address the unique content of infection prevention. Option B (meeting with the facility’s leadership) is valuable for understanding organizational priorities and gaining support, but it is more about collaboration and context-setting rather than direct preparation for presenting educational material. Option D (administering tuberculin skin tests to orientees) is a clinical task related to TB screening, not a preparatory activity for designing or delivering an educational presentation.
The focus on reviewing adult learning principles aligns with CBIC’s emphasis on evidence-based education strategies to improve infection control practices among healthcare personnel (CBIC Practice Analysis, 2022, Domain IV: Education and Research, Competency 4.2 - Evaluate the effectiveness of educational programs). This approach enables the IP to effectively communicate critical information, such as hand hygiene or isolation protocols, during the orientation program.
References: CBIC Practice Analysis, 2022, Domain IV: Education and Research, Competencies 4.1 - Develop and implement educational programs, 4.2 - Evaluate the effectiveness of educational programs.
Respiratory tract flora are BEST characterized by which of the following statements?
The airway is sterile below the larynx
Both the upper and lower airways are sterile throughout
Both the upper and lower airways contain small numbers of organisms
The upper airway is heavily colonized while the lower airway is not
The respiratory tract flora refers to the microbial communities inhabiting the respiratory system, and understanding their distribution is essential for infection prevention and diagnosis. The Certification Board of Infection Control and Epidemiology (CBIC) highlights the importance of microbial ecology in the "Identification of Infectious Disease Processes" domain, which aligns with the Centers for Disease Control and Prevention (CDC) and clinical microbiology principles. The question seeks the best characterization of respiratory tract flora, requiring an evaluation of current scientific understanding.
Option C, "Both the upper and lower airways contain small numbers of organisms," is the most accurate statement. The upper respiratory tract (e.g., nasal passages, pharynx) is naturally colonized by a diverse microbial community, including bacteria like Streptococcus, Staphylococcus, and Corynebacterium, as well as some fungi and viruses, acting as a first line of defense. The lower respiratory tract (e.g., trachea, bronchi, alveoli) was traditionally considered sterile due to mucociliary clearance and immune mechanisms. However, recent advances in molecular techniques (e.g., 16S rRNA sequencing) have revealed a low-biomass microbiome in the healthy lower airway, consisting of small numbers of organisms such as Prevotella and Veillonella, likely introduced via microaspiration from the upper tract. The CDC and studies in journals like the American Journal of Respiratory and Critical Care Medicine (e.g., Dickson et al., 2016) support this view, indicating that both regions contain microbial populations, though the lower airway’s flora is less dense and more tightly regulated.
Option A, "The airway is sterile below the larynx," is outdated. While the lower airway was once thought to be sterile, modern research shows a sparse microbial presence, debunking this as a complete characterization. Option B, "Both the upper and lower airways are sterile throughout," is incorrect. The upper airway is clearly colonized, and the lower airway, though low in microbial load, is not entirely sterile. Option D, "The upper airway is heavily colonized while the lower airway is not," overstates the contrast. The upper airway is indeed heavily colonized, but the lower airway is not sterile; it contains small numbers of organisms rather than being completely free of microbes.
The CBIC Practice Analysis (2022) and CDC guidelines on respiratory infections acknowledge the evolving understanding of respiratory flora, emphasizing that both upper and lower airways host small microbial populations in healthy individuals. Option C best reflects this balanced and evidence-based characterization.
References:
CBIC Practice Analysis, 2022.
Dickson, R. P., et al. (2016). The Microbiome and the Respiratory Tract. American Journal of Respiratory and Critical Care Medicine.
CDC Principles of Epidemiology, 3rd Edition, 2012.
Which of the following stains is used to identify mycobacteria?
Acid-fast
Gram
Methylene blue
India ink
Mycobacteria, including species such as Mycobacterium tuberculosis and Mycobacterium leprae, are a group of bacteria known for their unique cell wall composition, which contains a high amount of lipid-rich mycolic acids. This characteristic makes them resistant to conventional staining methods and necessitates the use of specialized techniques for identification. The acid-fast stain is the standard method for identifying mycobacteria in clinical and laboratory settings. This staining technique, developed by Ziehl-Neelsen, involves the use of carbol fuchsin, which penetrates the lipid-rich cell wall of mycobacteria. After staining, the sample is treated with acid-alcohol, which decolorizes non-acid-fast organisms, while mycobacteria retain the red color due to their resistance to decolorization—hence the term "acid-fast." This property allows infection preventionists and microbiologists to distinguish mycobacteria from other bacteria under a microscope.
Option B, the Gram stain, is a common differential staining technique used to classify most bacteria into Gram-positive or Gram-negative based on the structure of their cell walls. However, mycobacteria do not stain reliably with the Gram method due to their thick, waxy cell walls, rendering it ineffective for their identification. Option C, methylene blue, is a simple stain used to observe bacterial morphology or as a counterstain in other techniques (e.g., Gram staining), but it lacks the specificity to identify mycobacteria. Option D, India ink, is used primarily to detect encapsulated organisms such as Cryptococcus neoformans by creating a negative staining effect around the capsule, and it is not suitable for mycobacteria.
The CBIC’s "Identification of Infectious Disease Processes" domain underscores the importance of accurate diagnostic methods in infection control, including the use of appropriate staining techniques to identify pathogens like mycobacteria. The acid-fast stain is specifically recommended by the CDC and WHO for the initial detection of mycobacterial infections, such as tuberculosis, in clinical specimens (CDC, Laboratory Identification of Mycobacteria, 2008). This aligns with the CBIC Practice Analysis (2022), which emphasizes the role of laboratory diagnostics in supporting infection prevention strategies.
References:
CBIC Practice Analysis, 2022.
CDC Laboratory Identification of Mycobacteria, 2008.
WHO Guidelines for the Laboratory Diagnosis of Tuberculosis, 2014.
A healthcare worker experiences a percutaneous exposure to a patient with untreated HIV. The next step is to:
Initiate HIV post-exposure prophylaxis (PEP) within 2 hours.
Wait for HIV test results before starting treatment.
Offer post-exposure prophylaxis only if symptoms develop.
Retest for HIV after 6 months before deciding on PEP.
HIV post-exposure prophylaxis (PEP) should be initiated within 2 hours to be most effective.
Waiting for results (B) delays critical treatment.
PEP should always be offered after high-risk exposure, not only if symptoms develop (C).
Retesting after 6 months (D) is recommended but should not delay PEP initiation.
CBIC Infection Control References:
APIC Text, "Bloodborne Pathogens and PEP," Chapter 11.
Which of the following factors increases a patient’s risk of developing ventilator-associated pneumonia (VAP)?
Hypoxia
Nasogastric tube
Acute lung disease
In-line suction
Ventilator-associated pneumonia (VAP) is a type of healthcare-associated pneumonia that occurs in patients receiving mechanical ventilation for more than 48 hours. The Certification Board of Infection Control and Epidemiology (CBIC) emphasizes identifying risk factors for VAP in the "Prevention and Control of Infectious Diseases" domain, aligning with the Centers for Disease Control and Prevention (CDC) guidelines for preventing ventilator-associated events. The question requires identifying which factor among the options increases a patient’s risk of developing VAP, based on evidence from clinical and epidemiological data.
Option B, "Nasogastric tube," is the correct answer. The presence of a nasogastric tube is a well-documented risk factor for VAP. This tube can facilitate the aspiration of oropharyngeal secretions or gastric contents into the lower respiratory tract, bypassing natural defense mechanisms like the epiglottis. The CDC’s "Guidelines for Preventing Healthcare-Associated Pneumonia" (2004) and studies in the American Journal of Respiratory and Critical Care Medicine (e.g., Kollef et al., 2005) highlight that nasogastric tubes increase VAP risk by promoting microaspiration, especially if improperly managed or if the patient has impaired gag reflexes. This mechanical disruption of the airway’s protective barriers is a direct contributor to infection.
Option A, "Hypoxia," refers to low oxygen levels in the blood, which can be a consequence of lung conditions or VAP but is not a primary risk factor for developing it. Hypoxia may indicate underlying respiratory compromise, but it does not directly increase the likelihood of VAP unless associated with other factors (e.g., prolonged ventilation). Option C, "Acute lung disease," is a broad term that could include conditions like acute respiratory distress syndrome (ARDS), which may predispose patients to VAP due to prolonged ventilation needs. However, acute lung disease itself is not a specific risk factor; rather, it is the need for mechanical ventilation that elevates risk, making this less direct than the nasogastric tube effect. Option D, "In-line suction," involves a closed-system method for clearing respiratory secretions, which is designed to reduce VAP risk by minimizing contamination during suctioning. The CDC and evidence-based guidelines (e.g., American Thoracic Society, 2016) recommend in-line suction to prevent infection, suggesting it decreases rather than increases VAP risk.
The CBIC Practice Analysis (2022) and CDC guidelines prioritize identifying modifiable risk factors like nasogastric tubes for targeted prevention strategies (e.g., elevating the head of the bed to reduce aspiration). Option B stands out as the factor most consistently linked to increased VAP risk based on clinical evidence.
References:
CBIC Practice Analysis, 2022.
CDC Guidelines for Preventing Healthcare-Associated Pneumonia, 2004.
Kollef, M. H., et al. (2005). The Impact of Nasogastric Tubes on VAP. American Journal of Respiratory and Critical Care Medicine.
American Thoracic Society Guidelines on VAP Prevention, 2016.
The Infection Prevention and Control Committee is concerned about an outbreak of Serratia marcescens in the intensive care unit. If an environmental source is suspected, the BEST method to validate this suspicion is to
apply fluorescent gel.
use ATP system.
obtain surface cultures.
perform direct practice observation.
The correct answer is C, "obtain surface cultures," as this is the best method to validate the suspicion of an environmental source for an outbreak of Serratia marcescens in the intensive care unit (ICU). According to the Certification Board of Infection Control and Epidemiology (CBIC) guidelines, Serratia marcescens is an opportunistic gram-negative bacterium commonly associated with healthcare-associated infections (HAIs), often linked to contaminated water, medical equipment, or environmental surfaces in ICUs. Obtaining surface cultures allows the infection preventionist (IP) to directly test environmental samples (e.g., from sinks, ventilators, or countertops) for the presence of Serratia marcescens, providing microbiological evidence to confirm or rule out an environmental source (CBIC Practice Analysis, 2022, Domain II: Surveillance and Epidemiologic Investigation, Competency 2.2 - Analyze surveillance data). This method is considered the gold standard for outbreak investigations when an environmental reservoir is suspected, as it offers specific pathogen identification and supports targeted interventions.
Option A (apply fluorescent gel) is a technique used to assess cleaning efficacy by highlighting areas missed during disinfection, but it does not directly identify the presence of Serratia marcescens or confirm an environmental source. Option B (use ATP system) measures adenosine triphosphate (ATP) to evaluate surface cleanliness and organic residue, which can indicate poor cleaning practices, but it is not specific to detecting Serratia marcescens and lacks the diagnostic precision of cultures. Option D (perform direct practice observation) is valuable for assessing staff adherence to infection control protocols, but it addresses human factors rather than directly validating an environmental source, making it less relevant as the initial step in this context.
The focus on obtaining surface cultures aligns with CBIC’s emphasis on using evidence-based methods to investigate and control HAIs, enabling the IP to collaborate with the committee to pinpoint the source and implement corrective measures (CBIC Practice Analysis, 2022, Domain II: Surveillance and Epidemiologic Investigation, Competency 2.3 - Identify risk factors for healthcare-associated infections). This approach is supported by CDC guidelines for outbreak investigations, which prioritize microbiological sampling to guide environmental control strategies (CDC Guidelines for Environmental Infection Control in Healthcare Facilities, 2019).
References: CBIC Practice Analysis, 2022, Domain II: Surveillance and Epidemiologic Investigation, Competencies 2.2 - Analyze surveillance data, 2.3 - Identify risk factors for healthcare-associated infections. CDC Guidelines for Environmental Infection Control in Healthcare Facilities, 2019.
Which of the following statements describes the MOST important consideration of an infection preventionist when assessing the effectiveness of an infection control action plan?
Re-evaluate the action plan every three years.
Update the plan before the risk assessment is completed.
Develop a timeline and assign responsibilities for the stated action.
Monitor and validate the related outcome and process measures.
Assessing the effectiveness of an infection control action plan is a critical responsibility of an infection preventionist (IP) to ensure that interventions reduce healthcare-associated infections (HAIs) and improve patient safety. The Certification Board of Infection Control and Epidemiology (CBIC) highlights this process within the "Surveillance and Epidemiologic Investigation" and "Performance Improvement" domains, emphasizing the need for ongoing evaluation and data-driven decision-making. The Centers for Disease Control and Prevention (CDC) and other guidelines stress that the ultimate goal of an action plan is to achieve measurable outcomes, such as reduced infection rates, which requires systematic monitoring and validation.
Option D, "Monitor and validate the related outcome and process measures," is the most important consideration. Outcome measures (e.g., infection rates, morbidity, or mortality) indicate whether the action plan has successfully reduced the targeted infection risk, while process measures (e.g., compliance with hand hygiene or proper catheter insertion techniques) assess whether the implemented actions are being performed correctly. Monitoring involves continuous data collection and analysis, while validation ensures the data’s accuracy and relevance to the plan’s objectives. The CBIC Practice Analysis (2022) underscores that effective infection control relies on evaluating both outcomes (e.g., decreased central line-associated bloodstream infections) and processes (e.g., adherence to aseptic protocols), making this a dynamic and essential step. The CDC’s "Compendium of Strategies to Prevent HAIs" (2016) further supports this by recommending regular surveillance and feedback as key to assessing intervention success.
Option A, "Re-evaluate the action plan every three years," suggests a periodic review, which is a good practice for long-term planning but is insufficient as the most important consideration. Infection control requires more frequent assessment (e.g., quarterly or annually) to respond to emerging risks or outbreaks, making this less critical than ongoing monitoring. Option B, "Update the plan before the risk assessment is completed," is illogical and counterproductive. Updating a plan without a completed risk assessment lacks evidence-based grounding, undermining the plan’s effectiveness and contradicting the CBIC’s emphasis on data-driven interventions. Option C, "Develop a timeline and assign responsibilities for the stated action," is an important initial step in implementing an action plan, ensuring structure and accountability. However, it is a preparatory activity rather than the most critical factor in assessing effectiveness, which hinges on post-implementation evaluation.
The CBIC Practice Analysis (2022) and CDC guidelines prioritize outcome and process monitoring as the cornerstone of infection control effectiveness, enabling IPs to adjust strategies based on real-time evidence. Thus, Option D represents the most important consideration for assessing an infection control action plan’s success.
References:
CBIC Practice Analysis, 2022.
CDC Compendium of Strategies to Prevent Healthcare-Associated Infections, 2016.
A healthcare facility has installed a decorative water fountain in their lobby for the enjoyment of patients and visitors. What is an important issue for the infection preventionist to consider?
Children getting Salmonella enteritidis
Cryptosporidium growth in the fountain
Aerosolization of Legionella pneumophila
Growth of Acinetobacter baumannii
The installation of a decorative water fountain in a healthcare facility lobby introduces a potential environmental hazard that an infection preventionist must evaluate, guided by the Certification Board of Infection Control and Epidemiology (CBIC) principles and infection control best practices. Water features can serve as reservoirs for microbial growth and dissemination, particularly in settings with vulnerable populations such as patients. The key is to identify the most significant infection risk associated with such a water source. Let’s analyze each option:
A. Children getting Salmonella enteritidis: Salmonella enteritidis is a foodborne pathogen typically associated with contaminated food or water sources like poultry, eggs, or untreated drinking water. While children playing near a fountain might theoretically ingest water, Salmonella is not a primary concern for decorative fountains unless they are specifically contaminated with fecal matter, which is uncommon in a controlled healthcare environment. This risk is less relevant compared to other waterborne pathogens.
B. Cryptosporidium growth in the fountain: Cryptosporidium is a parasitic protozoan that causes gastrointestinal illness, often transmitted through contaminated drinking water or recreational water (e.g., swimming pools). While decorative fountains could theoretically harbor Cryptosporidium if contaminated, this organism requires specific conditions (e.g., fecal contamination) and is more associated with untreated or poorly maintained water systems. In a healthcare setting with regular maintenance, this is a lower priority risk compared to bacterial pathogens spread via aerosols.
C. Aerosolization of Legionella pneumophila: Legionella pneumophila is a gram-negative bacterium that thrives in warm, stagnant water environments, such as cooling towers, hot water systems, and decorative fountains. It causes Legionnaires’ disease, a severe form of pneumonia, and Pontiac fever, both transmitted through inhalation of contaminated aerosols. In healthcare facilities, where immunocompromised patients are present, aerosolization from a water fountain poses a significant risk, especially if the fountain is not regularly cleaned, disinfected, or monitored. The CBIC and CDC highlight Legionella as a critical concern in water management programs, making this the most important issue for an infection preventionist to consider.
D. Growth of Acinetobacter baumannii: Acinetobacter baumannii is an opportunistic pathogen commonly associated with healthcare-associated infections (e.g., ventilator-associated pneumonia, wound infections), often found on medical equipment or skin. While it can survive in moist environments, its growth in a decorative fountain is less likely compared to Legionella, which is specifically adapted to water systems. The risk of Acinetobacter transmission via a fountain is minimal unless it becomes a direct contamination source, which is not a primary concern for this scenario.
The most important issue is C, aerosolization of Legionella pneumophila, due to its potential to cause severe respiratory infections, its association with water features, and the heightened vulnerability of healthcare facility populations. The infection preventionist should ensure the fountain is included in the facility’s water management plan, with regular testing, maintenance, and disinfection to prevent Legionella growth and aerosol spread, as recommended by CBIC and CDC guidelines.
References:
CBIC Infection Prevention and Control (IPC) Core Competency Model (updated 2023), Domain IV: Environment of Care, which addresses waterborne pathogens like Legionella in healthcare settings.
CBIC Examination Content Outline, Domain III: Prevention and Control of Infectious Diseases, which includes managing environmental risks such as water fountains.
CDC Toolkit for Controlling Legionella in Common Sources of Exposure (2021), which identifies decorative fountains as a potential source of Legionella aerosolization.
Some pathogens live in the body and can be cultured, but do NOT elicit any response from the body’s defense mechanisms. This state is called:
Colonization
Infection
Latency
Contamination
The interaction between pathogens and the human body can take various forms, each with distinct immunological and clinical implications. The Certification Board of Infection Control and Epidemiology (CBIC) emphasizes understanding these states within the "Identification of Infectious Disease Processes" domain to guide infection prevention strategies. The question describes a scenario where pathogens are present, can be cultured (indicating viable organisms), but do not trigger a response from the body’s defense mechanisms, such as inflammation or immune activation. This requires identifying the appropriate microbiological state.
Option A, "Colonization," is the correct answer. Colonization occurs when microorganisms are present on or in the body (e.g., skin, mucous membranes, or gut) without causing harm or eliciting an immune response. These pathogens can be cultured, as they are alive and replicating, but they exist in a commensal or symbiotic relationship with the host, not provoking symptoms or defense mechanisms. Examples include normal flora like Staphylococcus epidermidis on the skin or Streptococcus salivarius in the oral cavity. The Centers for Disease Control and Prevention (CDC) defines colonization as the presence of microbes without tissue invasion or damage, distinguishing it from infection (CDC, "Principles of Epidemiology in Public Health Practice," 3rd Edition, 2012).
Option B, "Infection," is incorrect because it involves the invasion and multiplication of pathogens in body tissues, leading to an immune response, such as inflammation, fever, or antibody production. This contrasts with the question’s description of no defense mechanism response. Option C, "Latency," refers to a state where a pathogen (e.g., herpes simplex virus or Mycobacterium tuberculosis) remains dormant in the body after initial infection, capable of reactivation but not eliciting an active immune response during dormancy. However, latency implies a prior infection with a latent phase, whereas the question suggests a current, non-responsive state without prior infection context. Option D, "Contamination," describes the unintended presence of pathogens on inanimate objects or surfaces (e.g., medical equipment), not within the body, and does not align with the scenario of living, culturable pathogens in a host.
The CBIC Practice Analysis (2022) and CDC guidelines highlight colonization as a key concept in infection control, particularly in settings like hospitals where colonized patients can serve as reservoirs for potential infections. The absence of an immune response, as specified, aligns with the definition of colonization, making Option A the most accurate answer.
References:
CBIC Practice Analysis, 2022.
CDC Principles of Epidemiology in Public Health Practice, 3rd Edition, 2012.
An infection preventionist should collaborate with a public health agency in primary prevention efforts by:
Conducting outbreak investigations.
Performing surveillance for tuberculosis through tuberculin skin test.
Promoting vaccination of health care workers and patients.
Offering blood and body fluid post-exposure prophylaxis.
Primary prevention focuses on preventing the initial occurrence of disease or injury before it manifests, distinguishing it from secondary (early detection) and tertiary (mitigation of complications) prevention. The Certification Board of Infection Control and Epidemiology (CBIC) emphasizes the "Prevention and Control of Infectious Diseases" domain, which includes collaboration with public health agencies to implement preventive strategies, aligning with the Centers for Disease Control and Prevention (CDC) framework for infection prevention. The question requires identifying the activity that best fits primary prevention efforts.
Option C, "Promoting vaccination of health care workers and patients," is the correct answer. Vaccination is a cornerstone of primary prevention, as it prevents the onset of vaccine-preventable diseases (e.g., influenza, hepatitis B, measles) by inducing immunity before exposure. The CDC’s "Immunization of Health-Care Personnel" (2011) and "General Recommendations on Immunization" (2021) highlight the role of vaccination in protecting both healthcare workers and patients, reducing community transmission and healthcare-associated infections. Collaboration with public health agencies, which often oversee vaccination campaigns and supply distribution, enhances this effort, making it a proactive primary prevention strategy.
Option A, "Conducting outbreak investigations," is a secondary prevention activity. Outbreak investigations occur after cases are identified to control spread and mitigate impact, focusing on containment rather than preventing initial disease occurrence. The CDC’s "Principles of Epidemiology in Public Health Practice" (3rd Edition, 2012) classifies this as a response to an existing problem. Option B, "Performing surveillance for tuberculosis through tuberculin skin test," is also secondary prevention. Surveillance, including tuberculin skin testing, aims to detect latent or active tuberculosis early to prevent progression or transmission, not to prevent initial infection. The CDC’s "Guidelines for Preventing the Transmission of Mycobacterium tuberculosis" (2005) supports this as a screening tool. Option D, "Offering blood and body fluid post-exposure prophylaxis," is tertiary prevention. Post-exposure prophylaxis (e.g., for HIV or hepatitis B) is administered after potential exposure to prevent disease development, focusing on mitigating consequences rather than preventing initial exposure, as outlined in the CDC’s "Updated U.S. Public Health Service Guidelines" (2013).
The CBIC Practice Analysis (2022) and CDC guidelines prioritize vaccination as a primary prevention strategy, and collaboration with public health agencies amplifies its reach. Option C best reflects this preventive focus, making it the correct choice.
References:
CBIC Practice Analysis, 2022.
CDC Immunization of Health-Care Personnel, 2011.
CDC General Recommendations on Immunization, 2021.
CDC Principles of Epidemiology in Public Health Practice, 3rd Edition, 2012.
A 2-yoar-old girl is admitted with a fractured tibia. At birth, she was diagnosed with congenital cytomegalovirus (CMV). Which of the following barrier precautions is appropriate for healthcare personnel caring for her?
Wear masks and gloves
Wear gloves when handling body fluids
No barrier precautions are needed
Use gowns, masks, gloves, and a private room
Standard Precautions are sufficient for congenital cytomegalovirus (CMV), which means that gloves should be used when handling body fluids. CMV is primarily transmitted via direct contact with saliva, urine, or blood.
Why the Other Options Are Incorrect?
A. Wear masks and gloves – Masks are not necessary unless performing high-risk aerosol-generating procedures.
C. No barrier precautions are needed – Gloves are required when handling bodily fluids to prevent transmission.
D. Use gowns, masks, gloves, and a private room – CMV does not require Contact or Airborne Precautions.
CBIC Infection Control Reference
APIC guidelines state that CMV transmission is prevented using Standard Precautions, primarily with glove use for body fluid contact.
On January 31, the nursing staff of a long-term care facility reports that five out of 35 residents have developed high fever, nasal discharge, and a dry cough. The BEST diagnostic tool to determine the causative agent is:
Blood culture
Sputum culture
Nasopharyngeal swab
Legionella serology
The scenario describes a cluster of five out of 35 residents in a long-term care facility developing high fever, nasal discharge, and a dry cough, suggesting a potential respiratory infection outbreak. The Certification Board of Infection Control and Epidemiology (CBIC) emphasizes the "Identification of Infectious Disease Processes" and "Surveillance and Epidemiologic Investigation" domains, which require selecting the most appropriate diagnostic tool to identify the causative agent promptly. The Centers for Disease Control and Prevention (CDC) provides guidance on diagnostic approaches for respiratory infections, particularly in congregate settings like long-term care facilities.
Option C, "Nasopharyngeal swab," is the best diagnostic tool in this context. The symptoms—high fever, nasal discharge, and a dry cough—are characteristic of upper respiratory infections, such as influenza, respiratory syncytial virus (RSV), or other viral pathogens common in congregate settings. A nasopharyngeal swab is the gold standard for detecting these agents, as it collects samples from the nasopharynx, where many respiratory viruses replicate. The CDC recommends nasopharyngeal swabs for molecular testing (e.g., PCR) to identify viruses like influenza, RSV, or SARS-CoV-2, especially during outbreak investigations in healthcare facilities. The dry cough and nasal discharge align with upper respiratory involvement, making this sample type more targeted than alternatives. Given the potential for rapid spread among vulnerable residents, early identification via nasopharyngeal swab is critical to guide infection control measures.
Option A, "Blood culture," is less appropriate as the best initial tool. Blood cultures are used to detect systemic bacterial infections (e.g., bacteremia or sepsis), but the symptoms described are more suggestive of a primary respiratory infection rather than a bloodstream infection. While secondary bacteremia could occur, blood cultures are not the first-line diagnostic for this presentation and are more relevant if systemic signs (e.g., hypotension) worsen. Option B, "Sputum culture," is useful for lower respiratory infections, such as pneumonia, where productive cough and sputum production are prominent. However, the dry cough and nasal discharge indicate an upper respiratory focus, and sputum may be difficult to obtain from elderly residents, reducing its utility here. Option D, "Legionella serology," is specific for diagnosing Legionella pneumophila, which causes Legionnaires’ disease, typically presenting with fever, cough, and sometimes gastrointestinal symptoms, often in association with water sources. While possible, the lack of mention of pneumonia or water exposure, combined with the upper respiratory symptoms, makes Legionella serology less likely as the best initial test. Serology also requires time for antibody development, delaying diagnosis compared to direct sampling.
The CBIC Practice Analysis (2022) and CDC guidelines for outbreak management in long-term care facilities (e.g., "Prevention Strategies for Seasonal Influenza in Healthcare Settings," 2018) prioritize rapid respiratory pathogen identification, with nasopharyngeal swabs being the preferred method for viral detection. Given the symptom profile and outbreak context, Option C is the most effective and immediate diagnostic tool to determine the causative agent.
References:
CBIC Practice Analysis, 2022.
CDC Prevention Strategies for Seasonal Influenza in Healthcare Settings, 2018.
CDC Guidelines for the Prevention and Control of Outbreaks in Long-Term Care Facilities, 2015.
What inflammatory reaction may occur in the eye after cataract surgery due to a breach in disinfection and sterilization of intraocular surgical instruments?
Endophthalmitis
Bacterial conjunctivitis
Toxic Anterior Segment Syndrome
Toxic Posterior Segment Syndrome
The correct answer is C, "Toxic Anterior Segment Syndrome," as this is the inflammatory reaction that may occur in the eye after cataract surgery due to a breach in disinfection and sterilization of intraocular surgical instruments. According to the Certification Board of Infection Control and Epidemiology (CBIC) guidelines, Toxic Anterior Segment Syndrome (TASS) is a sterile, acute inflammatory reaction that can result from contaminants introduced during intraocular surgery, such as endotoxins, residues from improper cleaning, or chemical agents left on surgical instruments due to inadequate disinfection or sterilization processes (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.3 - Ensure safe reprocessing of medical equipment). TASS typically presents within 12-48 hours post-surgery with symptoms like pain, redness, and anterior chamber inflammation, and it is distinct from infectious causes because it is not microbial in origin. A breach in reprocessing protocols, such as failure to remove detergents or improper sterilization, is a known risk factor, making it highly relevant to infection prevention efforts in surgical settings.
Option A (endophthalmitis) is an infectious inflammation of the internal eye structures, often caused by bacterial or fungal contamination, which can also result from poor sterilization but is distinguished from TASS by its infectious nature and longer onset (days to weeks). Option B (bacterial conjunctivitis) affects the conjunctiva and is typically a surface infection unrelated to intraocular surgery or sterilization breaches of surgical instruments. Option D (toxic posterior segment syndrome) is not a recognized clinical entity in the context of cataract surgery; inflammation in the posterior segment is more commonly associated with infectious endophthalmitis or other conditions, not specifically linked to reprocessing failures.
The focus on TASS aligns with CBIC’s emphasis on ensuring safe reprocessing to prevent adverse outcomes in surgical patients, highlighting the need for rigorous infection control measures (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.5 - Evaluate the environment for infection risks). This is supported by CDC and American Academy of Ophthalmology guidelines, which identify TASS as a preventable complication linked to reprocessing errors (CDC Guidelines for Disinfection and Sterilization, 2019; AAO TASS Task Force Report, 2017).
References: CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competencies 3.3 - Ensure safe reprocessing of medical equipment, 3.5 - Evaluate the environment for infection risks. CDC Guidelines for Disinfection and Sterilization in Healthcare Facilities, 2019. AAO TASS Task Force Report, 2017.
The cleaning and disinfection process that is appropriate for a particular surgical instrument depends on
all surgical instruments are cleaned and sterilized in the same manner.
instruments contaminated with blood must be bleach cleaned first.
the device manufacturer's written instructions for use.
the policies of the sterile processing department.
The correct answer is C, "the device manufacturer's written instructions for use," as this is the factor that determines the appropriate cleaning and disinfection process for a particular surgical instrument. According to the Certification Board of Infection Control and Epidemiology (CBIC) guidelines, the reprocessing of surgical instruments must follow the specific instructions provided by the device manufacturer to ensure safety and efficacy. These instructions account for the instrument’s material, design, and intended use, specifying the appropriate cleaning agents, disinfection methods, sterilization techniques, and contact times to prevent damage and ensure the elimination of pathogens (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.3 - Ensure safe reprocessing of medical equipment). This is also mandated by regulatory standards, such as those from the Food and Drug Administration (FDA) and the Association for the Advancement of Medical Instrumentation (AAMI), which require adherence to manufacturer guidelines to maintain device integrity and patient safety.
Option A (all surgical instruments are cleaned and sterilized in the same manner) is incorrect because different instruments have unique characteristics (e.g., materials like stainless steel vs. delicate optics), necessitating tailored reprocessing methods rather than a one-size-fits-all approach. Option B (instruments contaminated with blood must be bleach cleaned first) is a misconception; while blood contamination requires thorough cleaning, bleach is not universally appropriate and may damage certain instruments unless specified by the manufacturer. Option D (the policies of the sterile processing department) may guide internal procedures but must be based on and subordinate to the manufacturer’s instructions to ensure compliance and effectiveness.
The emphasis on manufacturer instructions aligns with CBIC’s focus on evidence-based reprocessing practices to prevent healthcare-associated infections (HAIs) and protect patients (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.5 - Evaluate the environment for infection risks). Deviating from these guidelines can lead to inadequate sterilization or instrument damage, increasing infection risks.
References: CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competencies 3.3 - Ensure safe reprocessing of medical equipment, 3.5 - Evaluate the environment for infection risks. AAMI ST79:2017, Comprehensive guide to steam sterilization and sterility assurance in health care facilities.
Which of the following measures has NOT been demonstrated to reduce the risk of surgical site infections?
Limiting the duration of preoperative hospital stay
Using antimicrobial preoperative scrub by members of the surgical team
Assuring adequate patient nutrition
Designating a specific surgical suite tor infected cases
There is no strong evidence that isolating infected cases in a separate surgical suite reduces SSI risk.
Step-by-Step Justification:
SSI Prevention Strategies Supported by Evidence:
Preoperative hospital stay limitation reduces exposure to hospital-acquired pathogens.
Antimicrobial preoperative scrubs lower bacterial load on the skin.
Adequate nutrition improves immune function and wound healing.
Why Designating a Separate Surgical Suite Is Not Effective:
Operating room environmental controls (e.g., laminar airflow, sterilization protocols) are more important than suite designation.
No significant reduction in SSIs has been observed by segregating infected cases into specific OR suites.
Why Other Options Are Correct:
A. Limiting preoperative hospital stay: Reduces nosocomial bacterial exposure.
B. Antimicrobial preoperative scrub: Decreases skin flora contamination.
C. Assuring adequate patient nutrition: Enhances immune defense against infections.
CBIC Infection Control References:
APIC Text, "Surgical Site Infection Prevention Strategies".
Which of the following represents a class II surgical wound?
Incisions in which acute, nonpurulent inflammation are seen.
Incisional wounds following nonpenetrating (blunt) trauma.
Incisions involving the biliary tract, appendix, vagina, and oropharynx.
Old traumatic wounds with retained devitalized tissue.
Surgical wounds are classified by the Centers for Disease Control and Prevention (CDC) into four classes based on the degree of contamination and the likelihood of postoperative infection. This classification system, detailed in the CDC’s Guidelines for Prevention of Surgical Site Infections (1999), is a cornerstone of infection prevention and control, aligning with the Certification Board of Infection Control and Epidemiology (CBIC) standards in the "Prevention and Control of Infectious Diseases" domain. The classes are as follows:
Class I (Clean): Uninfected operative wounds with no inflammation, typically closed primarily, and not involving the respiratory, alimentary, genital, or urinary tracts.
Class II (Clean-Contaminated): Operative wounds with controlled entry into a sterile or minimally contaminated tract (e.g., biliary or gastrointestinal), with no significant spillage or infection present.
Class III (Contaminated): Open, fresh wounds with significant spillage (e.g., from a perforated viscus) or major breaks in sterile technique.
Class IV (Dirty-Infected): Old traumatic wounds with retained devitalized tissue or existing clinical infection.
Option A, "Incisions in which acute, nonpurulent inflammation are seen," aligns with a Class II surgical wound. The presence of acute, nonpurulent inflammation suggests a controlled inflammatory response without overt infection, which can occur in clean-contaminated cases where a sterile tract (e.g., during elective gastrointestinal surgery) is entered under controlled conditions. The CDC defines Class II wounds as those involving minor contamination without significant spillage or infection, and nonpurulent inflammation fits this category, often seen in early postoperative monitoring.
Option B, "Incisional wounds following nonpenetrating (blunt) trauma," does not fit the Class II definition. These wounds are typically classified based on the trauma context and are more likely to be considered contaminated (Class III) or dirty (Class IV) if there is tissue damage or delayed treatment, rather than clean-contaminated. Option C, "Incisions involving the biliary tract, appendix, vagina, and oropharynx," describes anatomical sites that, when surgically accessed, often fall into Class II if the procedure is elective and controlled (e.g., cholecystectomy), but the phrasing suggests a general category rather than a specific wound state with inflammation, making it less precise for Class II. Option D, "Old traumatic wounds with retained devitalized tissue," clearly corresponds to Class IV (dirty-infected) due to the presence of necrotic tissue and potential existing infection, which is inconsistent with Class II.
The CBIC Practice Analysis (2022) emphasizes the importance of accurate wound classification for implementing appropriate infection prevention measures, such as antibiotic prophylaxis or sterile technique adjustments. The CDC guidelines further specify that Class II wounds may require tailored interventions based on the observed inflammatory response, supporting Option A as the correct answer. Note that the phrasing in Option A contains a minor grammatical error ("inflammation are seen" should be "inflammation is seen"), but this does not alter the clinical intent or classification.
References:
CBIC Practice Analysis, 2022.
CDC Guidelines for Prevention of Surgical Site Infections, 1999.